Obesity in America
In 2013, 38% of US adults and 17% of US children were classified as obese. During this time, the American Medical Association recognized obesity as a disease. It is to no surprise that obesity increases the risk of other comorbidities such as diabetes, heart disease, stroke, arthritis, and some cancers (1).
Defining Obesity with BMI
Body mass index (BMI) is a great resource and quick do-it-yourself assessment of your weight status. The table below classifies your weight status by using your BMI. If you do not know your BMI, you can enter your weight and height into the National Institutes of Health BMI calculator.
| Definition | BMI (kg/m2) |
|
Underweight |
Below 18.5 |
| Normal | 18.5–24.9 |
| Overweight | 25.0–29.9 |
| Obesity | 30.0 and Above |
As convenient as it is to use BMI, it has some significant limitations. BMI does not take muscle mass into account which could be problematic for athletes who have a great deal of muscle because muscle weighs more than fat! Athletes often have higher BMI scores and can wrongfully be classified as overweight or even obese. Older populations must also take caution with their BMI score. BMI tends to underestimate body fat in the elderly population. With that being said, be aware that BMI is a rough estimate of your weight status. For example, a football player with a BMI of 27 kg/m2 would technically be classified as overweight. However, are they really overweight or do they just have a lot of muscle mass?
Guide to Selecting Treatment
Overweight and obesity can often be targeted and successfully managed with diet, exercise, and behavior therapy. The next line of defense, particularly for those with a BMI > 27 kg/m2, is medication prescribed by your doctor. The last and most invasive treatment is for those with a BMI > 30 kg/m2, which involves bariatric surgery. It is important to remember that lifestyle changes are always the first line of defense! More times than not, these changes will help to bring you back to a healthy weight (2).
What is Bariatric Surgery?
“Bariatric surgery is an operation that helps you lose weight by making changes to your digestive system,” (3).
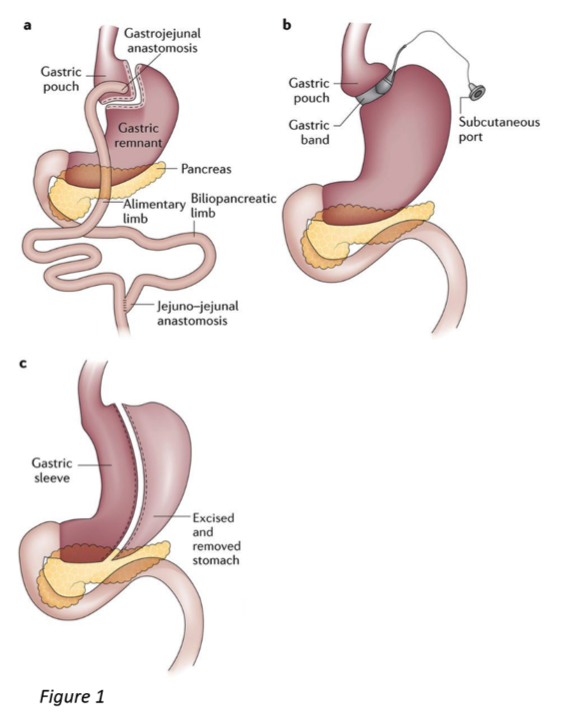
There are different procedures that change your digestive system in different ways. The most popular surgeries include (3):
- Laparoscopic Adjustable Gastric Banding (Figure 1b)
- Gastric Sleeve Surgery (Figure 1c)
- Roux-En Y Gastric Bypass (Figure 1a)
Bariatric surgery is a potential option for those who are obese, unable to lose weight or keep the weight off, and/or suffering from serious health problems, such as type 2 diabetes (3).
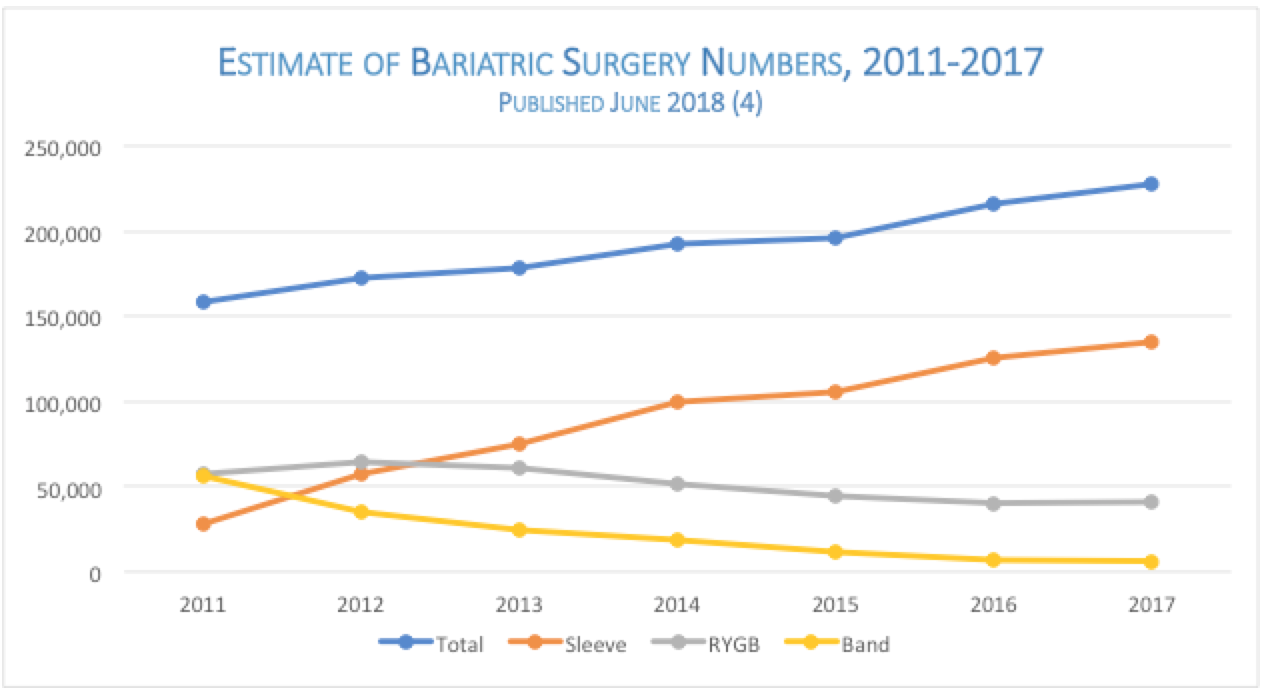
The ASMBS total bariatric procedure numbers are based on the best estimation from available data (BOLD,ACS/MBSAQIP, National Inpatient Sample Data and outpatient estimations)
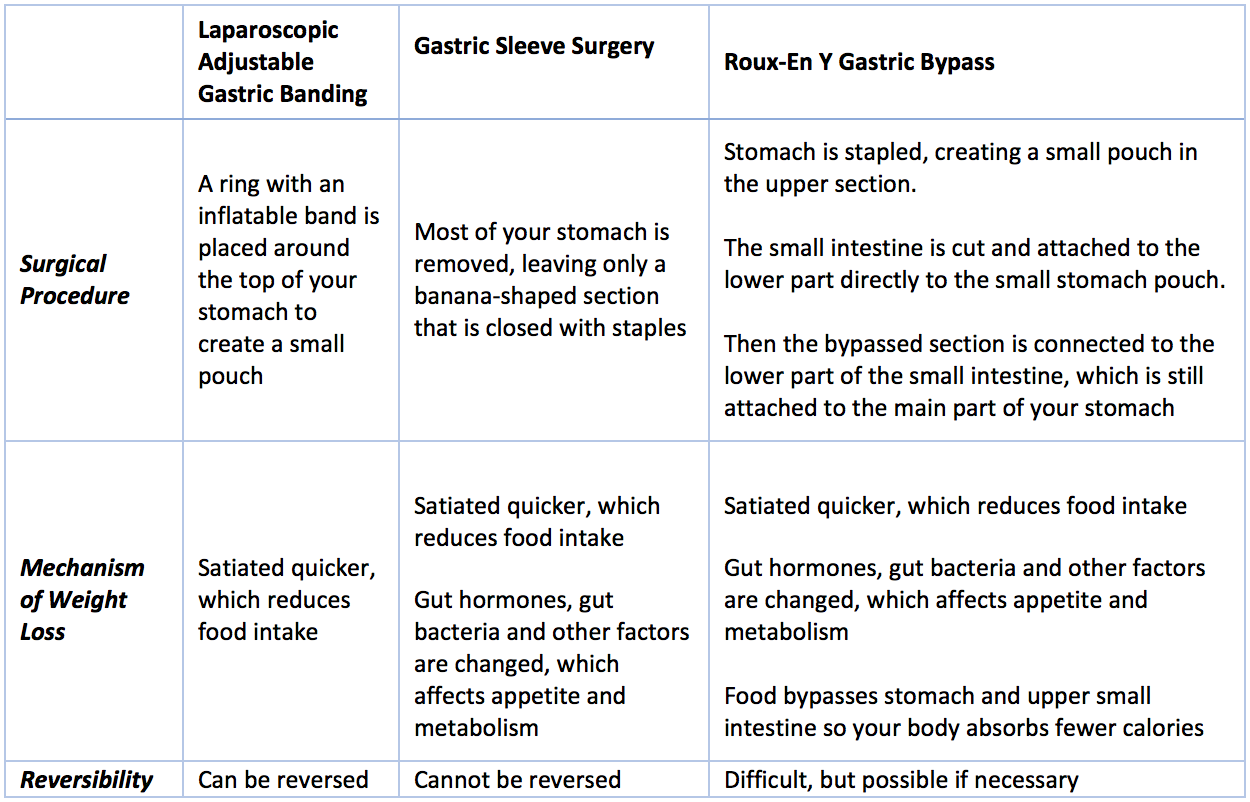
Commonly Performed Surgeries (3)
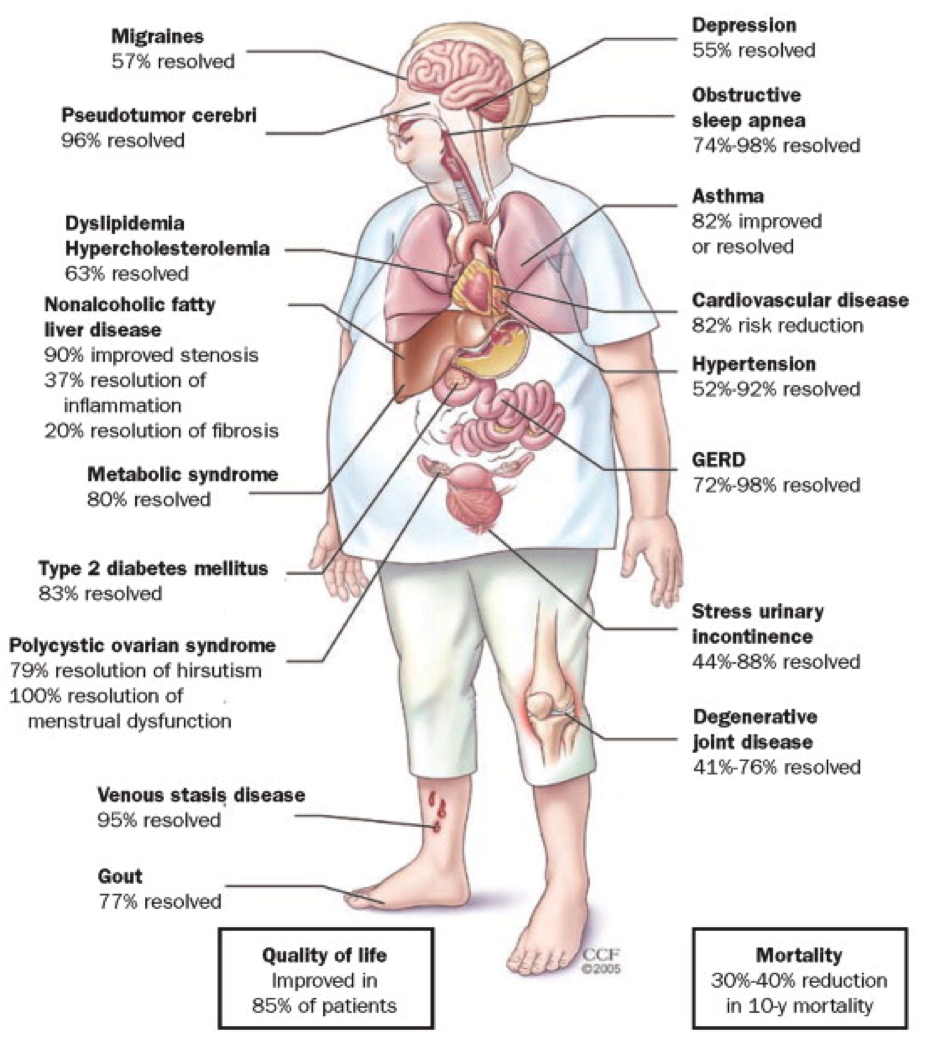
Resolution of Comorbidities After Bariatric Surgery (5)
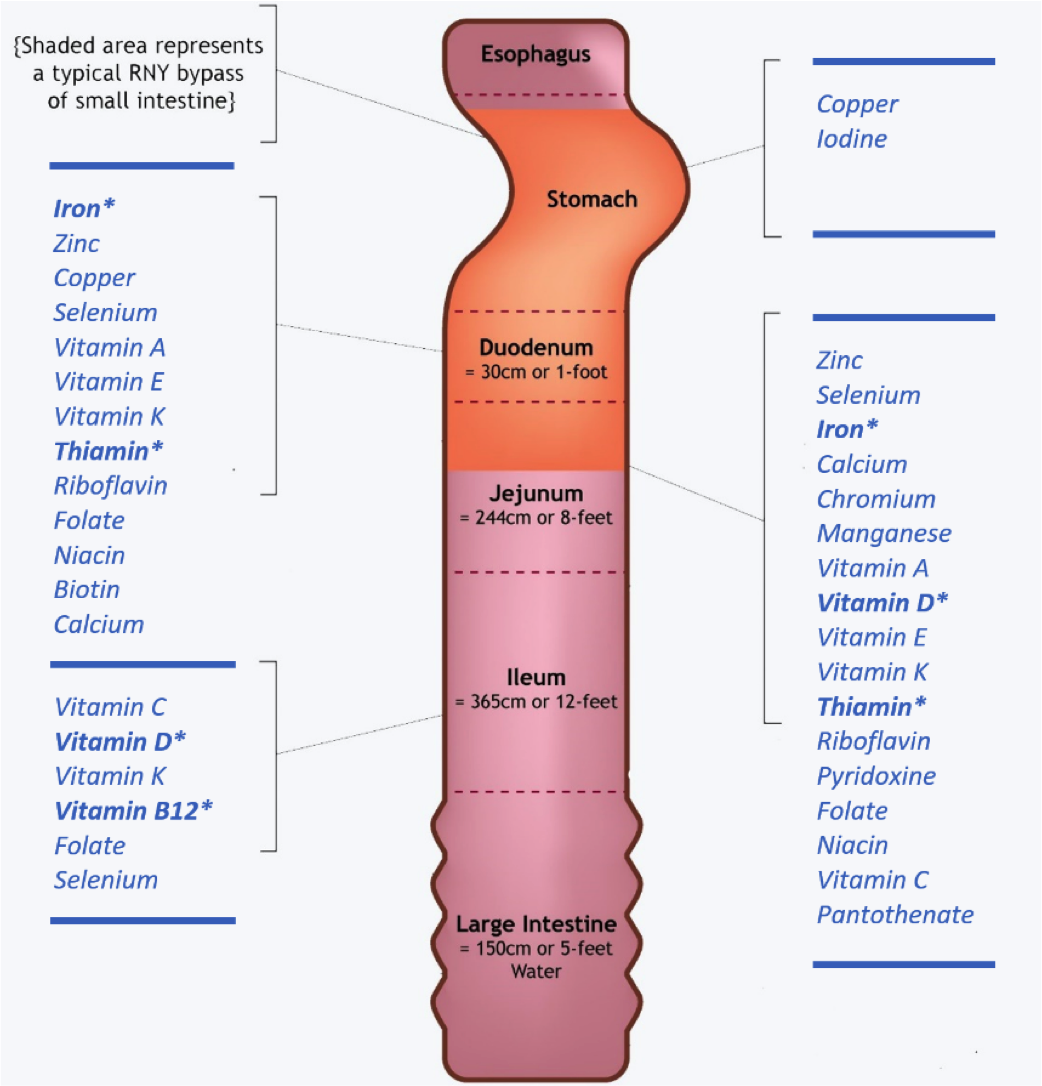
Micronutrient Absorption
Literature in Review
A 2018 systematic review and meta-analysis sought to evaluate the efficacy of vitamin D supplementation on the prevention of postoperative vitamin D deficiency and found that a daily dosage of more than 800 IU was effective in preventing deficiency and improving 25-OHD levels (6).
A randomized controlled trial investigated whether oral supplementation increases and normalizes low vitamin B12 concentrations in Roux-en Y gastric bypass patients compared to intramuscular injections. Participants randomly assigned to receive vitamin B12 orally, received daily doses of 1000 ug. Vitamin B12 was normalized in all individuals, which indicates that oral vitamin B12 supplementation can be used as an alternative to intramuscular injections, which are typically painful, and require a considerable amount of time and effort from patients and healthcare professionals (7).
A retrospective analysis of prospectively collected data was obtained from patients who underwent a Roux-en Y gastric bypass to assess the long-term outcome of nutritional status after surgery. A total of 35%, 16%, and 55% of the patients had deficiencies for iron, vitamin B12, and vitamin D, respectively. Furthermore, those who used a daily multivitamin had a lower rate of iron, vitamin B12, and vitamin D deficiency, compared to those who did not use a daily multivitamin (8).
Recommended Vitamin Supplementation
Liquid Calcium and Magnesium with 1000 IU of Vitamin D3
Physician’s Multi Vitamin Formula
Vitamin B-12 Triple Action Timed Release Formula
Additional Resources
https://medlineplus.gov/obesity.html
References
(1) Flegal KM, Kruszon-Moran D, Carroll MD, Fryar CD, Ogden CL. Trends in Obesity Among Adults in the United States, 2005 to 2014. JAMA. 2016; 315(21):2284.
(2) Persaud, A. Nutrition guidelines for bariatric surgery. Bariatric & Metabolic Services: Harlem Hospital. 2017 [PowerPoint].
(3) Types of Bariatric Surgery | NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases Web site. https://www.niddk.nih.gov/health-information/weight-management/bariatric-surgery/types. Updated July 2016. Accessed August 13, 2018.
(4) Estimate of Bariatric Surgery Numbers, 2011-2017. American Society for Metabolic and Bariatric Surgery Web site. https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers. Accessed August 10, 2018.
(5) Schwartz SS, Kohl BA. Glycemic Control and Weight Reduction Without Causing Hypoglycemia: The Case for Continued Safe Aggressive Care of Patients With Type 2 Diabetes Mellitus and Avoidance of Therapeutic Inertia. Mayo Clinic Proceedings. 2010; 85(12):S15–26.
(6) Li Z, Zhou X, Fu W. Vitamin D Supplementation for the Prevention of Vitamin D Deficiency after Bariatric Surgery: A Systematic Review and Meta-Analysis. European Journal of Clinical Nutrition. 2018; 72(8):1061–70.
(7) Schijns W, Homan J, van der Meer L, Janssen IM, van Laarhoven CJ, Berends FJ, Aarts EO. Efficacy of Oral Compared with Intramuscular Vitamin B-12 Supplementation after Roux-En-Y Gastric Bypass: A Randomized Controlled Trial. The American Journal of Clinical Nutrition. 2018; 108(1):6–12.
(8) Dogan K, Homan J, Aarts EO, de Boer H, van Laarhoven CJ, Berends FJ. Long-Term Nutritional Status in Patients Following Roux-En-Y Gastric Bypass Surgery. Clinical Nutrition. 2018; 37(2):612–17.
Written by Nicole Lindel, MS in Nutrition Education from Columbia University